A new CDC study (inadvertently?) finds 28 times more fully vaccinated patients (5,213) were hospitalized with COVID from June to September than the unvaccinated with prior infection (189) in nine U.S. states.
The CDC was apparently hoping this study would demonstrate the superiority of vaccination relative to natural immunity from a prior infection so they could compel more Americans to get vaccinated. It may have backfired.
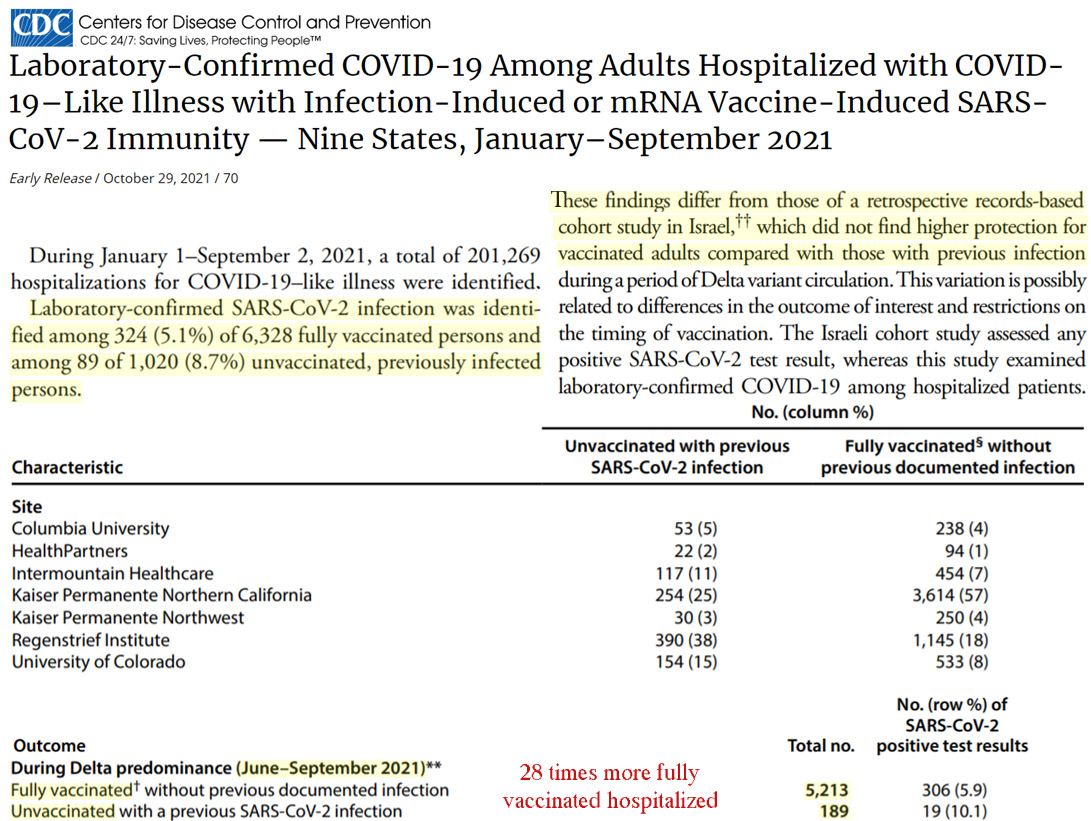
Image Source: CDC
Out of 201,269 people hospitalized with “COVID-19-like illness” from January to September (2021) in 9 states, just 1,020 (0.5%) of the hospitalizations occurred in unvaccinated people previously infected with COVID. This is a remarkably small number considering the CDC has estimated 120.2 million Americans (36.8% of the US population) had already been infected with COVID by late May.
Out of these 1,020 unvaccinated COVID patients landing in the hospital from January to September, 89 (8.7%) had tested positive for COVID a second time. The CDC interpreted this to mean natural immunity was less protective against re-infection with symptomatic COVID than vaccination because the percentage of infected fully vaccinated people in the hospital was 5.1%, or 1.7 times less.
But the rather hidden internals of the paper reveal a remarkable statistic: there were 27.6 times more (5,213 vs. 189) fully vaccinated than unvaccinated patients with COVID who needed to be hospitalized from June to September. Considering the prevalence of infection in the U.S. (probably 40-45% of the U.S. population had been infected by June to September if prevalence was 37% by late May), there is little likelihood there were 28 times more people vaccinated than already infected. This would appear to contradict the very vaccination-reduces-hospitalization conclusion the CDC had intended to emphasize in the first place.
UK: 90% of new infections and 89% of deaths over 70 are in the fully vaccinated
During weeks 38 to 41 (October), 2021, the UK Health Security Agency reports there were 117,882 of 130,904 (90%) new COVID cases identified in people aged 40 to 49 years old and fully vaccinated.
And the fully vaccinated were 2.2 times more likely to be infected with COVID (1,731.3 vs. 772.9 new cases per 100,000) than the unvaccinated in the 40-49 age group. Also, the fully vaccinated were about 2 times more likely to be infected in age groups 50-59, 60-69, and 70-79. It was only in the under 30 age groups that the unvaccinated had higher infection rates than the vaccinated.
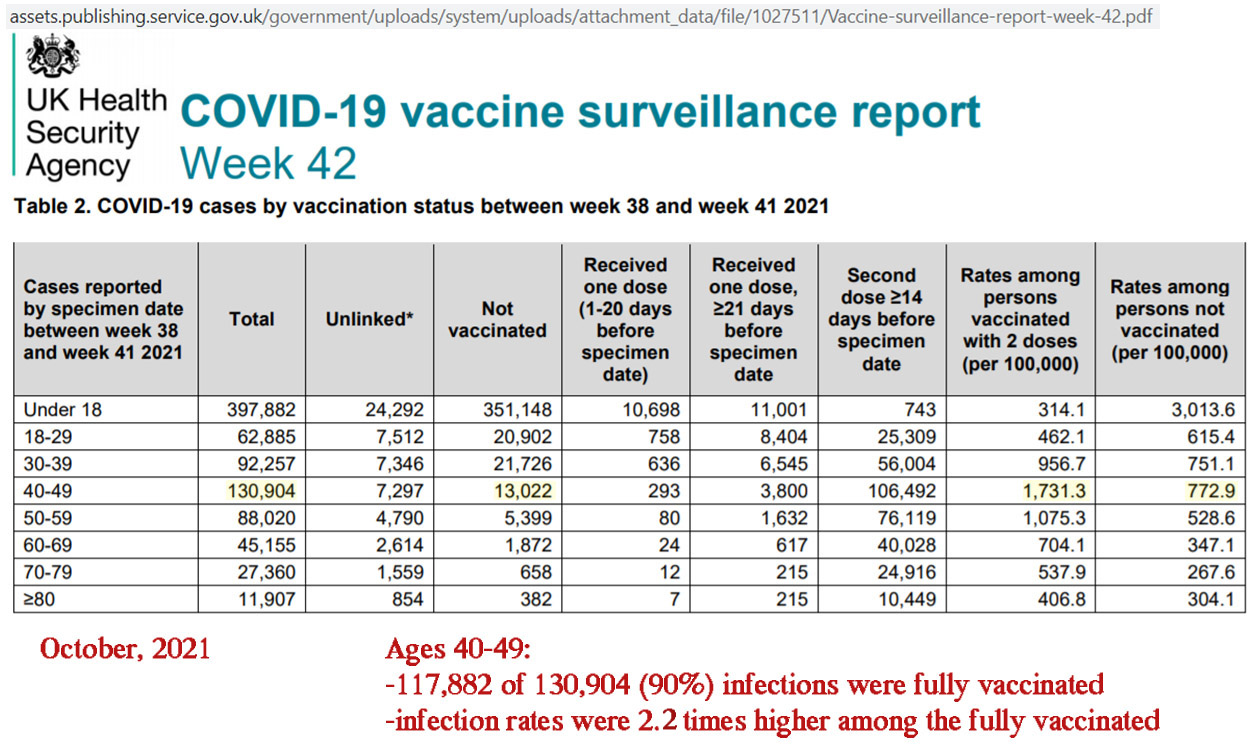
Image Source: UK Health Security Agency
The latest report for weeks 39 to 42 indicates 2,333 of 2,621 (89%) COVID deaths were in the fully vaccinated. Again, that’s nearly 9 of every 10 deaths.
This death percentage is slightly lower than the percentage of 70+ fully vaccinated (more than 90%), and thus the UKHSA has emphasized that the unvaccinated are more at risk with regard to probabilities. But this is little consolation in defending vaccine effectiveness when 89% of those dying are fully vaccinated.
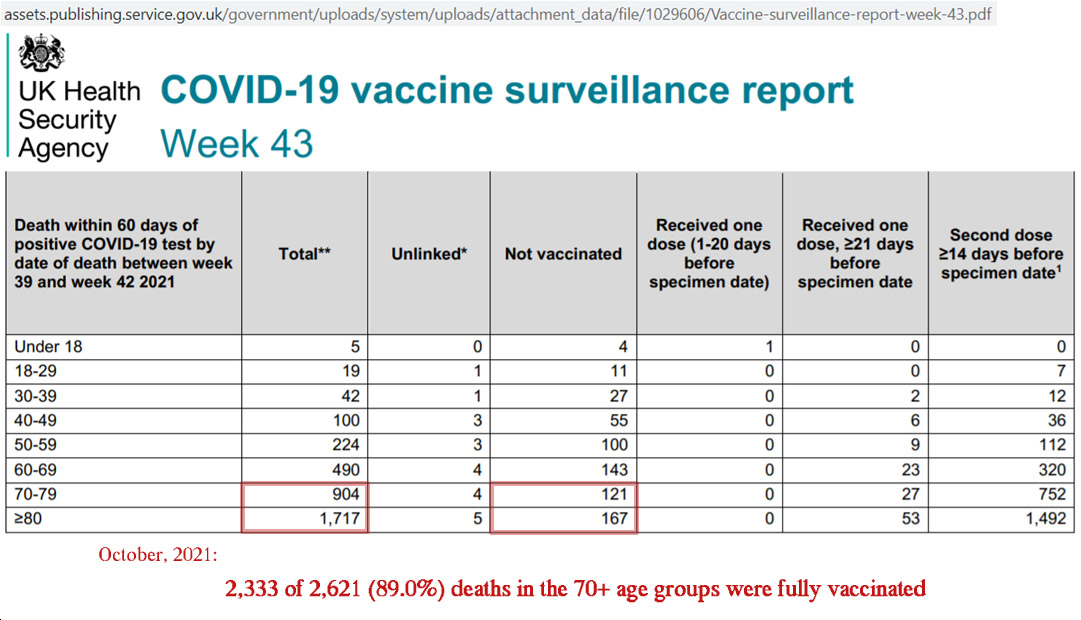
Image Source: UK Health Security Agency
3 studies find vaccine effectiveness vanishes to 0% after 5-7 months
In a study on vaccine effectiveness in hundreds of thousands of Qatar residents we learn that protection against infection peaks at 72.1% 4 to 5 weeks after the second dose, and then it rapidly declines to 0% (i.e., no more protection than the unvaccinated) within 140 days, or 20 weeks and later.
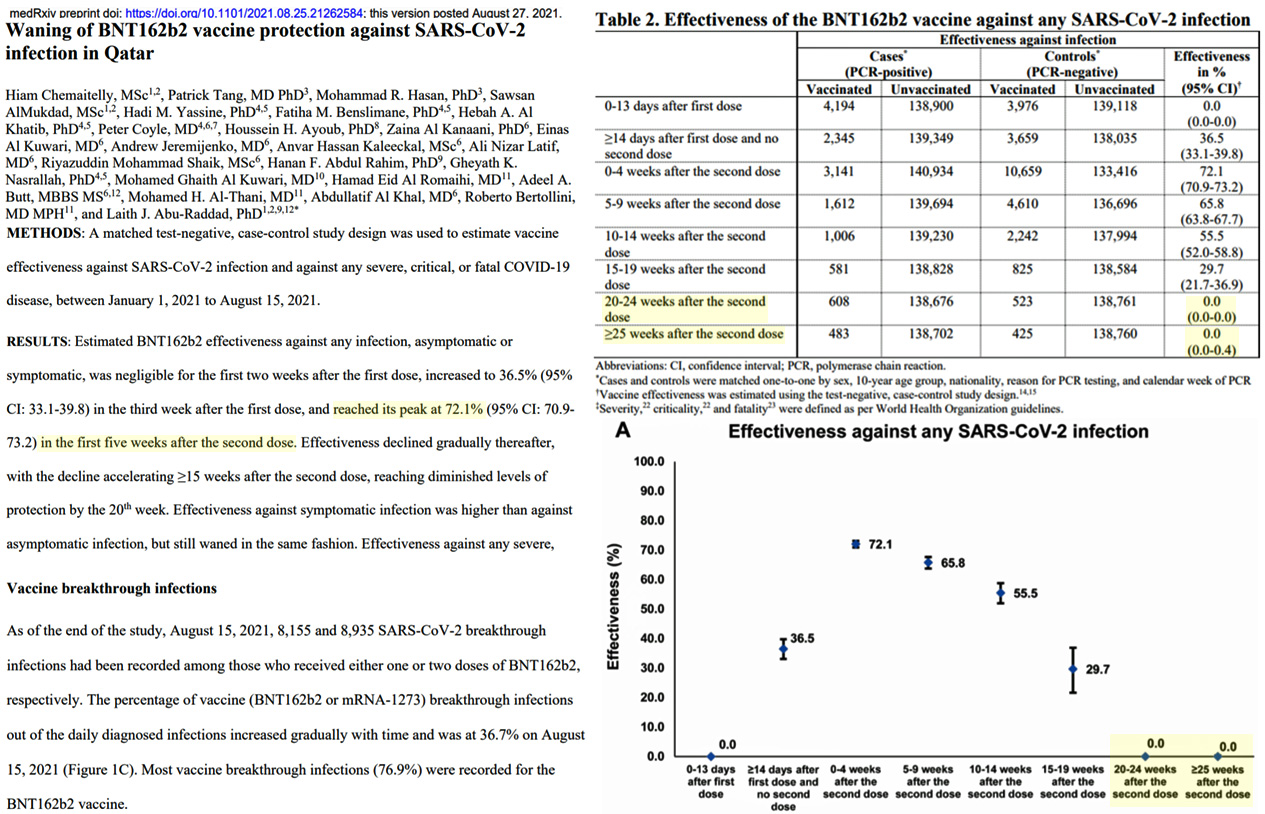
Image Source: Chemaitelly et al., 2021
Another study analyzed 11,889 infections in Israel and found infectiousness protection among the fully vaccinated “vanished” to the point there was no distinguishing the vaccinated from the unvaccinated within 180 days.
“[T]he viral load effectiveness declines with time post vaccination, significantly decreasing already after 3 months and effectively vanishing after about six months.”
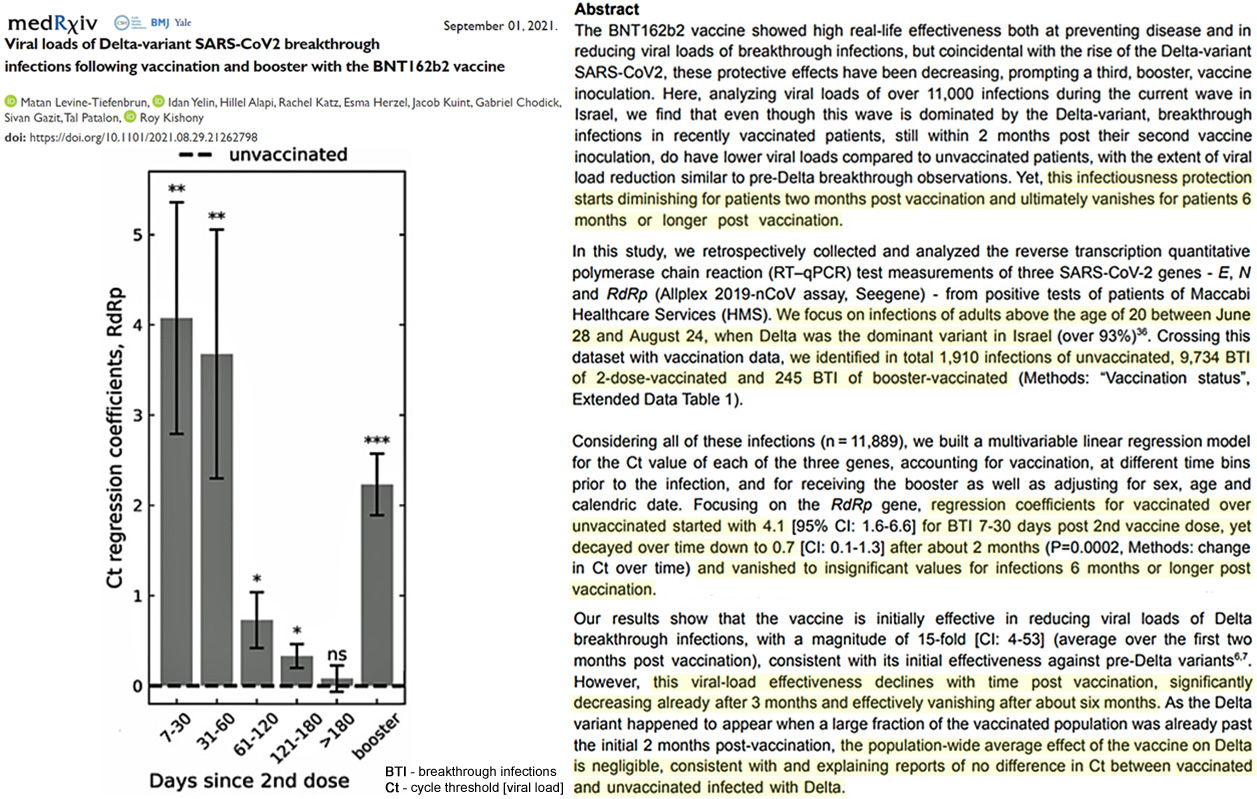
Image Source: Levine-Tiefenbrun et al., 2021
A nation-wide study of Sweden’s mass vaccination campaign determined that vaccine effectiveness fell from 92% to 47% within 121-180 days after the second shot, and then “from day 211 and onwards no effectiveness could be detected.”
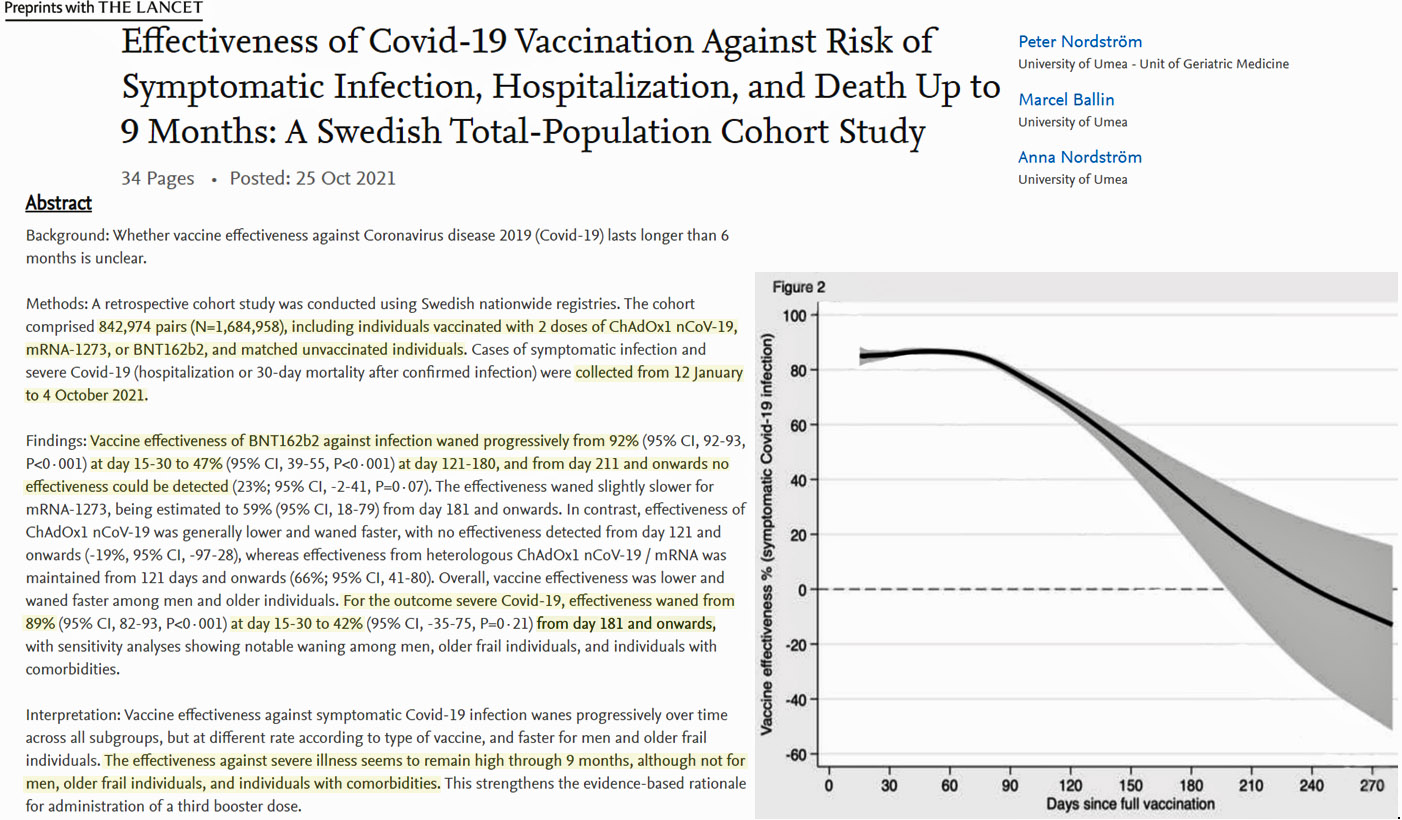
Image Source: Nordström et al., 2021
A disturbing study of 582 vaccine recipients (health care workers) found 48.4% were infected with COVID within 4 weeks after their first shot, and 25.3% were infected with COVID within 3 months after their second shot. It’s as if these vaccines offer no protection at all.
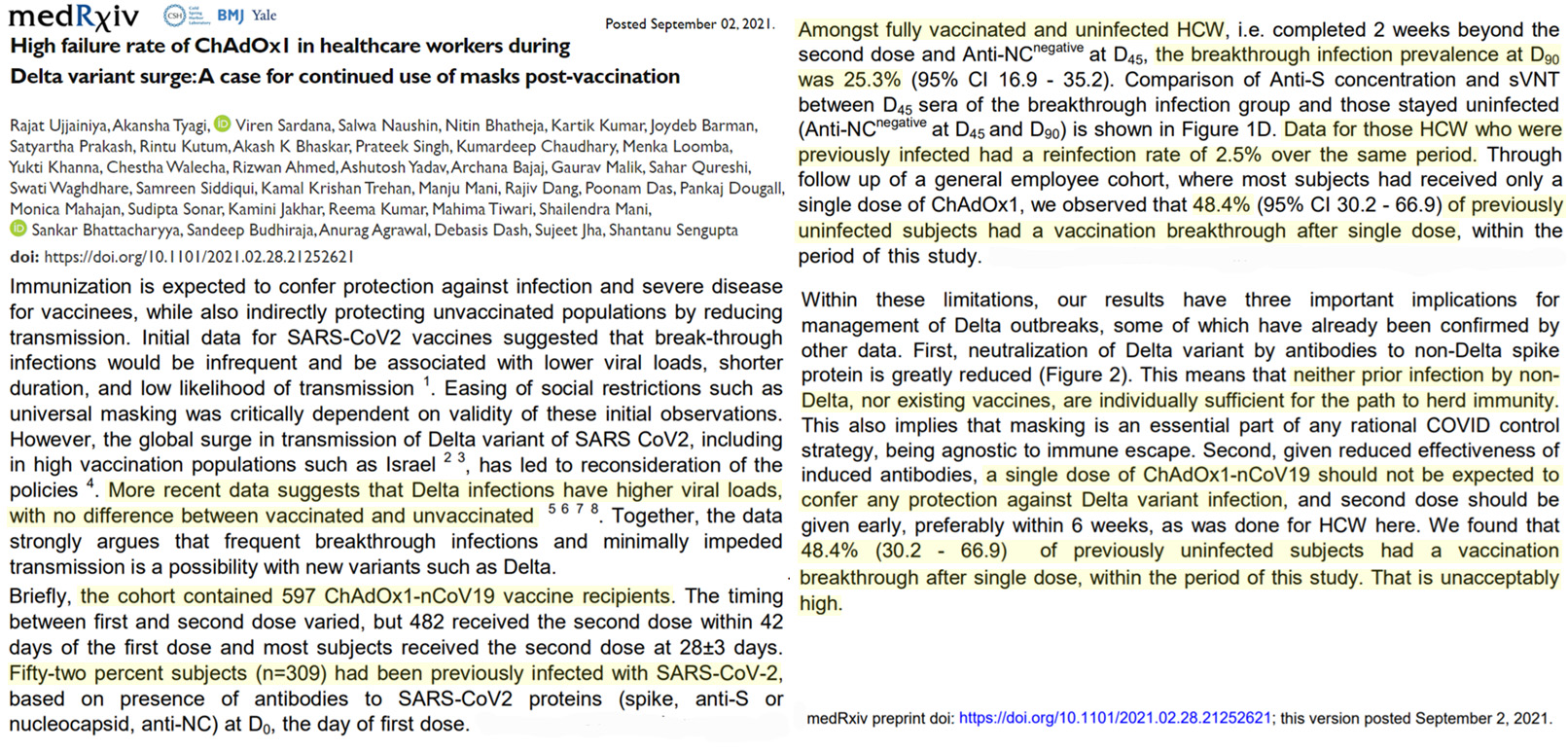
Image Source: Ujjainiya et al., 2021
Natural immunity from a prior infection is better than vaccines
In contrast to the rapidly-waning protection offered by COVID’s “leaky” vaccines, a collection of 96 studies (as of 1 November) and counting compiled by an epidemiologist and 5 other MDs affirm a prior COVID infection (i.e., natural immunity) offers more and longer-lasting protection than vaccines do.
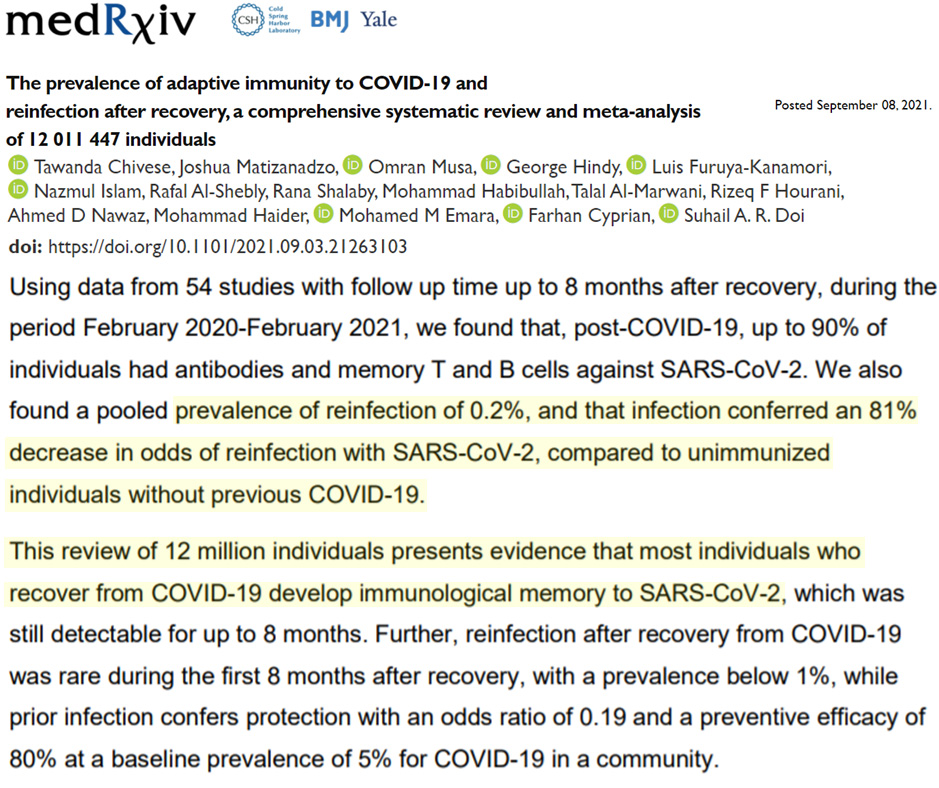
For example, according to a compendium of 54 studies involving over 12 million people, those who have already been infected with COVID are re-infected at a rate of only 0.2% (1 in 500) in the next 8 months after infection.

https://dailysceptic.org/2021/10/30/hide-the-vaccine-failure-ukhsa-caves-to-pressure-and-removes-chart-showing-higher-infection-rates-in-the-vaccinated-as-effectiveness-hits-new-low-of-minus-132/
They’re starting to hide this information.
“An outbreak of common colds at an Antarctic base after seventeen weeks of complete isolation”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2130424/
how are these respiratory diseases transmitted, what triggers them and why do some people not get ill.
This is a job for the much lauded Space Defense – monitor cometary RNA influx!
Considering photosynthesis started with a viral ‘infection’ resulting in a ‘champagne’ oxygen event killing all anaerobic life forms giving us our fossil resources, and our current biosphere, and now we find cometary dust may be bringing more RNA into the biosphere – it is indeed a serious scientific question for various space programs like NASA.
This natural process could exterminate us or show how we must advance – that is science in action.
They caught a cold. Common cold is not an infectous disease. You get it through exposure to cold weather. Everybody can do the experiment.
Baloney. Skiers spend a lot of time in cold weather
and they seem like a healthy bunch of people.
Baloney is that it’s infectous. If you spend a lot of time in cold weather, you acclimate, harden off and become more resistant. If you do this a lot, you become very healthy, assuming healthy food and physical activity. If you don’t, the first prolonged exposure to cold weather, and you catch a cold, or worse… Like I said, everybody can do this experiment.
In the above link, the evidence is that it happened after 2 weeks of very bad weather conditions. They caught a cold.
From the link:
“Inoculation of a pool of nasal secretions from these volunteers into a further seven volunteers produced no symptoms”
It is staying indoors in cold weather that is linked to respiratory infections, not the cold weather itself. The same happens in tropical regions when it is too hot to go outdoors.
Respiratory diseases spread best indoors and in the winter many people have lower levels of Vitamin D. Both explain the seasonal trend which also applies to COVID — in the US, COVID deaths were quite low in summer 2020, and in Summer 2021.
Worth reading.
https://www.spiked-online.com/2020/10/19/the-danger-of-scientific-dogmatism/
“Hope-Simpson further suggested that the speed of movement of epidemics is therefore unaffected by the speed and complexity of human communications (an idea that, if applied to a coronavirus, would also challenge the conventional tale of Covid-19’s spread from Wuhan in China through human travel).”
“Covid-19: Researcher blows the whistle on data integrity issues in Pfizer’s vaccine trial”
https://www.bmj.com/content/375/bmj.n2635
Besides the obvious HUGE flaw:
Only two months of testing
fully vaccinated people before EUA.
Tests with monkeys also only lasted two months,
which was just enough time to measure
COVID antibody counts (near their peak).
Two months is not a test.
Tests take several years.
Exactly.
The cure is worse than the disease, whether it’s lockdowns or these worthless and harmful so-called vaccines.
And let’s not forget that we are facing a pandemic of side effects to the vaccines.
What we have here is relative risk, which can be deceptive. To assess absolute risk we need to know the number of fully vaccinated and also the number of unvaccinated with prior infection in the population the hospital serves.
maybe this could be of use.
https://trialsitenews.com/pfizer-biontech-fail-to-report-low-absolute-risk-reduction-in-covid-19-booster-vaccine-trial-results/
And a big thank you to all that work at this site- it’s always on look everyday basis.
Relative risk reduction was 95%
Absolute risk reduction was about1%
Which number would YOU use to sell vaccines?
The mere two months of testing
catching the vaccines
at their peak effectiveness
which declines rapidly after a few months.
But, but, but these injection are effective — aren’t they?
https://www.bitchute.com/video/QbWq47ij8bNz/
They are very effective
at making profits
for drug companies.
Vaccination has never stop infection. Not smallpox, not chicken pox, not polio although some were inoculations. What they did was reduce the effect of the disease.
It is true that they also reduced transmission. The problem with the virus is that it is mostly likely man made and therefore somewhat prone to mutation. If we allow ourselves to search for herd immunity through death and serious illness will they provide a breeding ground for a seriously volatile and dangerous mutation. Will the vaccine reduce this risk. I don’t know the answers and should we accept the risk ?
The Categorical Imperative for viri is “You cannot kill your host.” Now this may be an exception because it has had some engineering, but is it universally lethal? Apparently not, so the Categorical Imperative must still be in force.
Polio and smallpox vaccines were very effective.
All viruses are prone to mutation.
They tend to mutate into less deadly variants.
Here’s a very informative interview that is, IMO, a goldmine of infection and “vaccine” information.
https://evidencenotfear.com/tag/dr-robert-malone/
They cover some of the topics, or aspects thereof, in Kenneth’s selection of papers, and more.
“The latest report for weeks 39 to 42 indicates 2,333 of 2,621 (89%) COVID deaths were in the fully vaccinated. Again, that’s nearly 9 of every 10 deaths”
The table above suggests only ~2% of 70-79 year olds and ~3% of over 80’s are unvaccinated.
So it looks like you’re between 3 – 5 times more likely to die if unvaccinated.
Some unvaccinated have natural antibodies,
In the UK the medical authorities have estimated
that 98% of people age 60+ have antibodies, eith
natural or vaccine induced.
Most deaths are in the age 60+ category.
If the vaccinated are working as promised
there should be very few deaths of vaccinated people.
Remember that deaths in the five week from
the first of two shots, and two weeks after
the last shot may be defined as unvaccinated
(that is true in the uS)
Almost alk deaths caused by the vaccines
are in the two weeks after the injection,
which could be defined as unvaccinated deaths.
(that is also true in the US.
The vaccines are not working well
after the first few months as
antibody counts decline much faster
than natural antibodies.
The vaccine adverse side effects would have
caused any other vaccine prior to 2020
to be halted by government authorities.
Apparently no bureaucrats care in 2021.
Covid-19: Researcher blows the whistle on data integrity issues in Pfizer’s vaccine trial
“”I don’t think it was good clean data,” the employee said of the data Ventavia generated for the Pfizer trial. “It’s a crazy mess.”
A second employee also described an environment at Ventavia unlike any she had experienced in her 20 years doing research. She told The BMJ that, shortly after Ventavia fired Jackson, Pfizer was notified of problems at Ventavia with the vaccine trial and that an audit took place.
Since Jackson reported problems with Ventavia to the FDA in September 2020, Pfizer has hired Ventavia as a research subcontractor on four other vaccine clinical trials (covid-19 vaccine in children and young adults, pregnant women, and a booster dose, as well an RSV vaccine trial…”
https://www.bmj.com/content/375/bmj.n2635?utm_source=twitter&utm_medium=social&utm_term=hootsuite&utm_content=sme&utm_campaign=usage
Italian Institute Of Health Drastically Reduces Its Official COVID Death Toll Number
https://www.zerohedge.com/markets/italian-institute-health-drastically-reduces-its-official-covid-death-toll-number
Italy was pretty much ground zero for the “Pandemic”, and the fact that they have reduced their official number of fatalities by 97% is highly significant.
Misinterpretation of data.
COVID and influenza can lead to deaths
from failures of major organs, usually lungs,
(almost always accompanied by other
pre-existing medical problems from obesity
to heart disease.)
For example:
In 2019, what used to be called
a US death FROM heart disease,
WITH influenza
as a contributory factor
… has been redefined for COVID
(by the US CDC in March 2020)
to be death FROM COVID,
with heart disease
as a contributory factor
(believe it or not).
That’s a very different way of counting deaths
WITH COVID versus deaths WITH influenza,
that is dishonest, in my opinion.
The headline of this story is misleading. It should say unvaxed previously infected. It is clarified further down the page. Just saying.
Seeing this article prompted me to check the UK Health Security Agency (an oxymoron) covid surveillance reports and I am astonished to find they have changed their reporting method. Table 2 in these reports has shown and infection rate for vaccinated and unvaccinated. These rates show that the infection rate is higher in the vaccinated group than the unvaccinated, and the infection rate is increasing with time. A rather inconvenient fact, so now from week 43 they have removed the infection rates and just show total numbers which don’t tell us anything. A lesson in how to lie with statistics.